Thomas R. Henry, MD, MINCEP Epilepsy Care & University of Minnesota Comprehensive Epilepsy Center
Two types of brain electrical stimulation have been developed as alternatives to resective-ablative epilepsy surgery (removing or laser-ablating a part of the brain where seizures start), for patients whose seizures cannot be controlled with medications. The U.S. Food & Drug Administration approved the Responsive Cortical Stimulation (RNS®) system, produced by NeuroPace, in 2013. The F.D.A. approved Thalamic Deep Brain Stimulation for epilepsy, produced by Medtronic, in 2018. Both stimulation systems were extensively studied in clinical trials lasting many years before FDA approval (1,2).
The two types of brain stimulation each were approved for focal epilepsy, but differ in supposed mechanisms of action, in generator and stimulation locations, in open-loop versus closed-loop operation, and many other respects.
The closed-loop RNS® mechanism is thought to terminate seizure discharges by stimulating directly at the seizure onset zone(s). The RNS® system can be used to stimulate one or two sites in the brain where seizures start. Surface cortical sites can be stimulated through “subdural” electrodes that are placed by a neurosurgeon on the surface of the brain, while the hippocampus and other deep brain sites can be stimulated through “depth” electrodes that enter the brain tissue. The RNS® system also continuously records brain electrical activity through these electrodes. Recorded bursts of electrical activity that are electrographic seizures trigger a pre-programmed stimulation at the site of seizure onset. Electrical recording and stimulation are controlled by a small neurostimulator device which is implanted on the surface of the skull, under the scalp. The FDA approved the RNS® system for treatment of adults with partial-onset seizures that were not controlled with two or more antiepileptic drugs, that have been localized to no more than two foci with diagnostic testing, and that are frequent and disabling (motor partial seizures, complex partial seizures, and generalized tonic-clonic seizures).
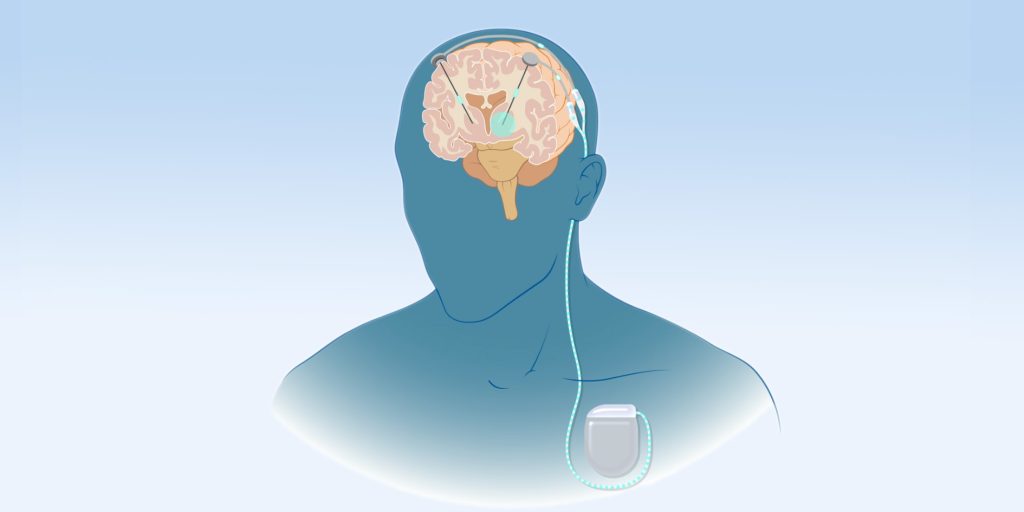
The open-loop thalamic stimulation mechanism (DBS) neuromodulates by stimulating the cells of the anterior thalamic nuclei which then project widely to areas in the frontal and temporal lobes. This thalamic stimulation acts to terminate seizure discharges or to reduce epileptic excitability in the seizure onset zone(s) that are distant from the thalamic nuclei. Cables run under the skin to connect to the generator near the clavicle. Intermittent trains of thalamic stimulation occur throughout the waking and sleeping hours. There is no continuous recording of brain electrical activity that can be used to direct alteration of the stimulation parameters during seizures. The FDA approved thalamic stimulation for treatment of adults with partial-onset seizures, with or without secondary generalization, who were not controlled with three or more antiepileptic drugs.
For both types of brain stimulation systems, the neurostimulator is non-invasively programmed through a magnetic wand. This programming changes the current, frequency and other parameters for stimulation. The magnetic wand also transfers EEG data from the implanted neurostimulator to the programmer’s laptop computer for storage and analysis. RNS®, patients can upload their data to the NeuroPace archives directly from home, so the data can be used later to tune the detected activities to possibly more effective stimulation settings.
For both types of brain stimulation systems, experts at epilepsy centers typically see the patient in the clinic every 1-3 months in the first year, with longer intervals between later visits. Both systems significantly improve seizure control in carefully selected patients, with 75-80% of patients having a greater than 50% seizure reduction and up to 20% of the patients becoming seizure-free in the long-term study reports which analyze the results at time periods up to 7 -9 years post-implant (3,4). Patients continue on anti-seizure medications in addition to the stimulation device.
Resective-ablative epilepsy surgery is more effective than brain stimulation for some patients, particularly those with temporal lobe epilepsy or a single site of seizure onset. Cognitive or motor deficits may be caused by resection-ablation and may be permanent. The aim of epilepsy surgery planning is to avoid post-operative deficits. So, for patients in which deficits are likely, the brain stimulation treatment plan will often be preferred since significant, irreversible deficits due to these system implantations are rare. In general, high-level epilepsy centers have experts who optimize medication regimens, perform exhaustive evaluation adapted to the individual patient, and then recommend options appropriate to the individual. These options include a course of surgically-based therapy with resection-ablation, RNS, thalamic DBS, or some other approach. These highly individualized evaluations allow the patient and the epilepsy physician to have a robust discussion of the options best suited to them. Patients and their healthcare providers have reasons to be excited by the expanding opportunities of brain stimulation therapies to control their refractory epilepsy.
REFERENCES
1. Morrell MJ, RNS System in Epilepsy Study Group. Responsive cortical stimulation for the treatment of medically intractable partial epilepsy. Neurology 77(13):1295-304, 2011.
2. Fisher R, Salanova V, Witt T, Worth R, Henry T, et al. Electrical stimulation of the anterior nucleus of thalamus for treatment of refractory partial epilepsy. Epilepsia 51: 899-908, 2010.
3. Nair, DR et als. Nine year prospective safety and efficacy of brain-responsive neurostimulation for focal epilepsy. Neurology. 2020 Sep 1;95(9):e1244-e1256. doi: 10.1212/WNL.0000000000010154. Epub 2020 Jul 20. PMID: 32690786; PMCID: PMC7538230.
4. https://www.medtronic.com/us-en/healthcare-professionals/therapies-procedures/neurological/deep-brain-stimulation/indications/epilepsy/clinical-outcomes.html#:~:text=EFFECTIVENESS%20RESULTS&text=DBS%20for%20Epilepsy%20was%20shown,in%20seizure%20frequency%20from%20baseline.