
Authors: Kai J. Miller, M.D., Ph.D., pediatric neurosurgeon Mayo Clinic and Anthony L. Fine, M.D., pediatric epileptologist Mayo Clinic
This blog post is sponsored by Mayo Clinic.
The concept of epilepsy surgery dates back to prehistoric times, though our understanding of epilepsy and surgical techniques has evolved significantly since then. While most patients with epilepsy achieve good seizure control with medication, some do not. Approximately 30% of people with epilepsy do not have control of their seizures despite trying two or more medications. These individuals would be classified as having refractory or intractable epilepsy.
In individuals with refractory epilepsy, particularly focal epilepsy, surgical evaluation should be considered early. For example, patients with temporal lobe epilepsy, where there is agreement between EEG findings and a structural abnormality on an MRI, can have up to an 80% chance of seizure freedom with surgery.
Early epilepsy surgery in children can have a significant impact on development, quality of life, improved psychosocial outcomes, and reduced morbidity and mortality. Unfortunately, many of these patients are delayed in referral for epilepsy surgery. This can be due to many causes, including a delay in the epilepsy diagnosis, waiting for epilepsy to be “outgrown,” continued medication trials with low likelihood of success, lack of findings on imaging, and other patient factors such as a reluctance to undergo surgery.
In the only randomized controlled trial of epilepsy surgery versus medication management, surgery outperformed medications for temporal lobe epilepsy. At one year, 58% in the surgery group compared to 8% in the medical management group were free of seizures impairing awareness, and 38% of the surgical group versus 3% of the medical management group were free of all seizures. In another study looking at early epilepsy surgery versus medication therapy for mesial temporal lobe epilepsy (MTLE), 11 of 15 in the surgery group compared to 0 of 23 in the medical group were seizure-free at their two-year follow-up.
Top reasons to have your child seen at a comprehensive epilepsy center:
- Your child is less than 2 years old
- Your child’s epilepsy hasn’t been controlled within two years of onset or with use of two medications
- Your child experiences intolerable side effects from medication
- Your child has disabling seizures that disrupt daily life
- Your child’s brain imaging shows a focal abnormality to explain epilepsy
- Your child’s epilepsy is affecting their normal brain development
- Your child has an underlying condition that requires special dietary or medical management (for example, glucose transporter deficiency or Dravet syndrome)
Diagnosis and treatment evaluation
The evaluation for epilepsy surgery is typically a staged approach. During initial workup (“Phase 1”) of the evaluation for epilepsy surgery, brain wave activity is recorded from the scalp with an electroencephalogram (EEG), seizures are recorded, and doctors are better able to predict what part of the brain the seizures comes from (seizure onset zone). Imaging studies, which may include magnetic resonance imaging (MRI), positron emission tomography (PET) scan and Subtraction ictal single photon emission computed tomography co-registered to MRI (SISCOM), are used to help confirm or refine that hypothesis.
Other studies that can be performed to assist in diagnostic workup include transcranial magnetic stimulation (TMS), magnetoencephalography (MEG), and functional magnetic resonance imaging or functional MRI (fMRI). If these studies are in agreement with one another), the patient may be recommended to proceed with a surgical procedure following discussion at a multidisciplinary surgical epilepsy conference.
If the suspected seizure onset zone is in the eloquent cortex (areas of the brain that control important function, such as movement and speech), further non-invasive studies may be performed or it may be recommended that the patient undergo an implanted electrode study (“Phase 2”). Phase 2 consists of recording electrical activity in or on the surface of the brain to identify the seizure onset zone. Other reasons why Phase 2 intracranial monitoring could be recommended include a disagreement between scalp EEG and imaging findings, unclear scalp EEG findings, or if imaging is “negative” (doesn’t show an abnormality).
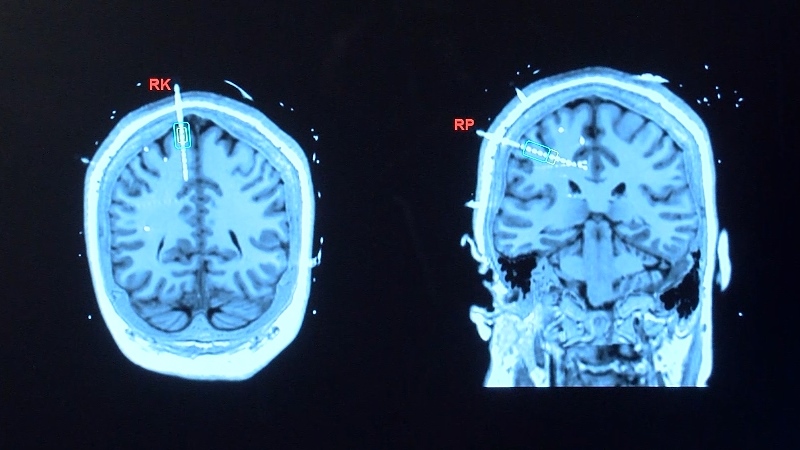
Stereoelectroencephalography (sEEG) records electrical signals within the brain by using electrodes that are implanted using a minimally invasive procedure. These electrodes help locate the seizure source when scalp EEG is unclear or the MRI is negative, but seizure activity is still suspected or observed. sEEG may also be used to map function in areas of the brain to be removed via resection or thermal ablation or to assess whether patients would benefit from implanted stimulation therapy.
sEEG is a less invasive method of obtaining recording. Many patients who undergo sEEG would have been monitored in the past with grid, strip, and depth electrodes that are placed on large areas of the brain surface; this involves a larger, “open” surgery where surgeons temporarily remove a large part of the skull bone and place grid and strip electrodes on the surface of the brain and penetrating depth electrodes into the brain.
In contrast, sEEG can be performed via small holes drilled in the skull. Anywhere from 10 to 15 electrode leads, with more than 200 electrode contacts, are typically placed during sEEG implantation, depending on the “hypothesis” for the location of the seizure onset zone. Some centers have robotic-assisted sEEG implantation, which can speed up implantation time. The typical hospitalization for sEEG monitoring is five to seven days, with some patients needing longer evaluations, and rarely some patients having a shorter evaluation.
Once sEEG is performed, most comprehensive epilepsy centers will bring together their multidisciplinary epilepsy team in a conference to evaluate and discuss treatment options. At Mayo Clinic, all surgical decisions are made on a consensus basis with teams of experts working together to form an individualized approach for each patient. Before any surgery, this team, which may include pediatric and adult epileptologists, neurosurgeons, and neuroradiologists, reviews all details of the patient’s history, imaging, and potential therapies before discussion with the patient and their family.
Minimally invasive surgical options
If there is a potential focus where seizure activity starts (seizure onset zone) that is not in a high risk area of the brain region, the patient may be a candidate for surgical resection, a procedure where part of the brain is removed that is causing seizures. A newer therapy to predict whether resection will reduce seizures is to perform radiofrequency ablation at the seizure onset zone through sEEG electrode contacts. Ablation is a less invasive type of epilepsy surgery where brain tissue is removed by either heat (thermal ablation) or soundwaves (radiofrequency). In some cases, patients can have a significant reduction in seizures without an open surgery, and, in others, a temporary reduction in seizures can forecast seizure freedom following resection.
Another type of thermal ablation, laser ablation, may be considered in place of focal open surgical resection. This can be helpful particularly when structures are far from the brain surface and difficult to reach surgically without passing through healthy brain. Radiofrequency and laser ablation can serve as less invasive initial steps, with resection still available, should these options fail.
FREQUENTLY ASKED QUESTIONS
Is surgery the best option for my child?
Patients may be surgical candidates if they continue to have seizures despite trying two or more medications, and their seizures are coming from one area of the brain. In individuals with epilepsy who have tried and failed two antiseizure medications, the chances of a third medication making them seizure free is less than 5%.
Should my child undergo sEEG for surgical evaluation?
For children with refractory epilepsy, sEEG may be helpful to localize the seizure source, particularly when scalp EEG is unclear and the MRI is negative. It may also be beneficial for evaluating and planning for surgery, helping the care team map out the area for resection and areas of the eloquent cortex. Additionally, sEEG can be used to evaluate candidacy for other treatments such as radiofrequency ablation or neurostimulation, including deep brain stimulation (DBS) and responsive neurostimulation (RNS).
What surgical intervention is best for my child?
Each individual child should be evaluated at a comprehensive epilepsy center. Every surgical decision should be individualized to fit a child’s unique situation, with the goal of improving seizures and minimizing side effects. When the seizures can be localized to a specific region (focal seizures), therapeutic options may include resection, ablation or implanted stimulator therapy (neuromodulation). If the seizures are generalized to the whole brain, or coming from more than one location, neuromodulation may be most appropriate. When seizures are medically-refractory and involve drop attacks (atonic) and/or frequent tonic seizures, corpus callosotomy (by laser or open surgery) may be appropriate.
About the authors:
Kai J. Miller, M.D., Ph.D., is a pediatric and adult neurosurgeon at Mayo Clinic who specializes in brain tumors, epilepsy, and deep-brain stimulation. He manages patients in both in the operating room and in the outpatient setting. His research involves measuring electrical brain activity with patients undergoing therapy with implanted electrodes, to understand brain circuit dynamics and develop new therapies. In addition to his active clinical and research programs, Dr. Miller teaches graduate students and mentors neurosurgical residents.
Anthony L. Fine, M.D., is a pediatric neurologist and epileptologist at Mayo Clinic. His clinical and research focus includes: Evaluation and treatment of epileptic encephalopathies, evaluation and treatment of ESES and the electroclinical syndromes of CSWS and LKS, diagnosis and management of genetic epilepsies and fetal and neonatal neurology. In addition, Dr. Fine is active in research and education, providing mentorship to residents and fellows.
About Mayo Clinic:
Mayo Clinic wants to make sure you feel empowered to make the right decisions for your care. The goals of treatment include no seizures, side effects or lifestyle limitations. You are at the center for your care, and Mayo Clinic’s team of multidisciplinary experts is ready to provide a personalized treatment plan for you. Beyond medications, Mayo’s teams of clinician researchers are on the cutting edge of new treatment options for people with seizure disorders. Advanced diagnostic technology help pinpoint the root cause of your seizures and help Mayo’s teams identify your best treatment options. Mayo’s top-ranked teams evaluate and treat more than 8,000 adult and pediatric patients with epilepsy each year. For more information or to request an appointment please visit mayoclinic.org/epilepsy.